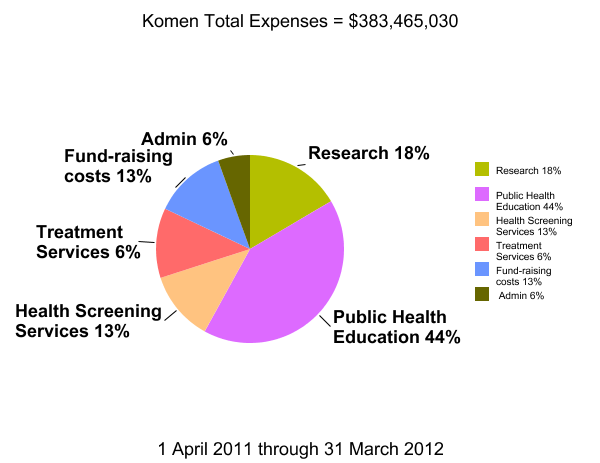
Figure 1. Total expenses of the Komen organization for the year ending 31 March 2012.
I love the Internet! With thanks to my friend GG, a stellar webcomber, I have been spending the last couple of days studying the most recent independent audit of the Susan G. Komen Breast Cancer Foundation, Inc. The audit is available to all as a PDF at that link.
First, the numbers
The Komen financial year runs from the first of April through March thirty-first. The most recent independently audited annual financial statement dates from March 31, 2012, and this post is based on those numbers.(*)

Figure 2. Gross breakdown of Total Expenses from Figure 1.
The good news first. Komen spends a relatively small portion of income on support services–about 19% of total expenses(the blue slice of the pie at the left). These support services expenses consist of fund-raising costs ($52,118,804 or 69%) and general/administrative costs ($23,064,504 or 31%).
The largest portion of Komen income, about 81%, is very appropriately spent on program expenses (the green slice). I am particularly interested in taking a closer look at how that $318,281,722 is spent.

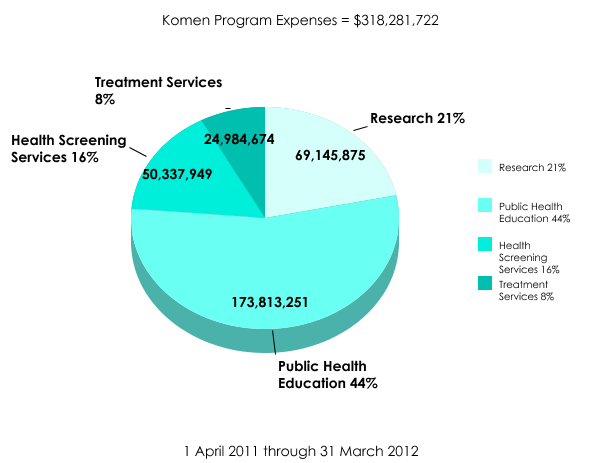
Figure 3. Breakdown of program expenses.
There are four categories of program expenses: Research (21% of total program expenses), Public Health Education (44%), Screening (16%) and Treatment Services (8%). The pie chart at the right shows the breakdown.
The lion’s share, of course, is spent on “public health education”. I assume this means awareness campaigns. About a fifth of program expenses are invested in research, approximately the same amount in health screen and treatment services.
Now the words
The Komen organization was founded in 1982. At that time it made enormous sense to make massive investment in public education and awareness, to dispel the fear that surrounded the word “cancer”. Young people today would have trouble understanding how terrifying the illness was; the word was rarely even pronounced aloud. People were too frightened to examine themselves and sometimes even to go to a doctor if they suspected something. After all, the reasoning went. It’s a death sentence whether I get treated or not.
So much has changed in the more than thirty years since that time. Cancer is now seen as a serious and treatable illness, rather than a death knell, and even metastatic cancer is approached as a chronic disease. Most women in the West have been taught about breast self-examination and breast exams are a regular part of the preventative medicine protocols of hospitals, clinics and insurers.
Moreover, today’s medical thinking and standard of practice is rethinking its approach to mammography, moving toward starting later and repeating less frequently in most cases. The American Cancer Society’s recommendations now call for:
- Yearly mammograms are recommended starting at age 40 and continuing for as long as a woman is in good health
- Clinical breast exam (CBE) about every 3 years for women in their 20s and 30s and every year for women 40 and over
- Women should know how their breasts normally look and feel and report any breast change promptly to their health care provider. Breast self-exam (BSE) is an option for women starting in their 20s.
Is the Komen mission still relevant in 2013?
I’d prefer to answer a slightly different question. Do we still need a large, well-known breast cancer charity in 2013?
Yes, of course. But as the world has changed since 1982, I suggest that the Komen organization’s mission should change. In a country where fewer and fewer people have access and the means to pay for medical care, I suggest that Komen is well placed to increase the proportion of income spent on treatment services. Perhaps individual treatment grants or matching funds or helping to pay for the operation of breast clinics could be considered.
I suggest that more of the organization’s income should be invested in research, both clinical research and basic research. The more we know about cancer, the better equipped we will be to treat it, perhaps even prevent it. I don’t have a personal stake in this; today’s research is not going to benefit me. But think of the generations it could help!
My proposal, then, would be more of a three-piece pie: a third of program expenses to public health education, a third to research and a third to treatment services. What do you think?
=====
(*)The pie charts were made with the free Create-A-Graph tool available in the Kids’ Zone of the American National Center for Education Statistics.
Discrepancies in totals are due to rounding off or to my own arithmetic incompetence. The original figures are can be seen at the link to the independent audit in the first paragraph of this post. I welcome comment and correction.